
Nephrotic syndrome is a complex clinical condition requiring a nuanced approach to diagnosis and treatment. Understanding its underlying causes, clinical manifestations, and biochemical changes is essential for effective management.
By Dr. T. Vishnu Murthy

Nephrotic Syndrome has historically been used in two distinct contexts:
1. As a histopathologic term for renal disease without inflammatory components.
2. To describe the clinical manifestation caused by substantial urinary protein loss.
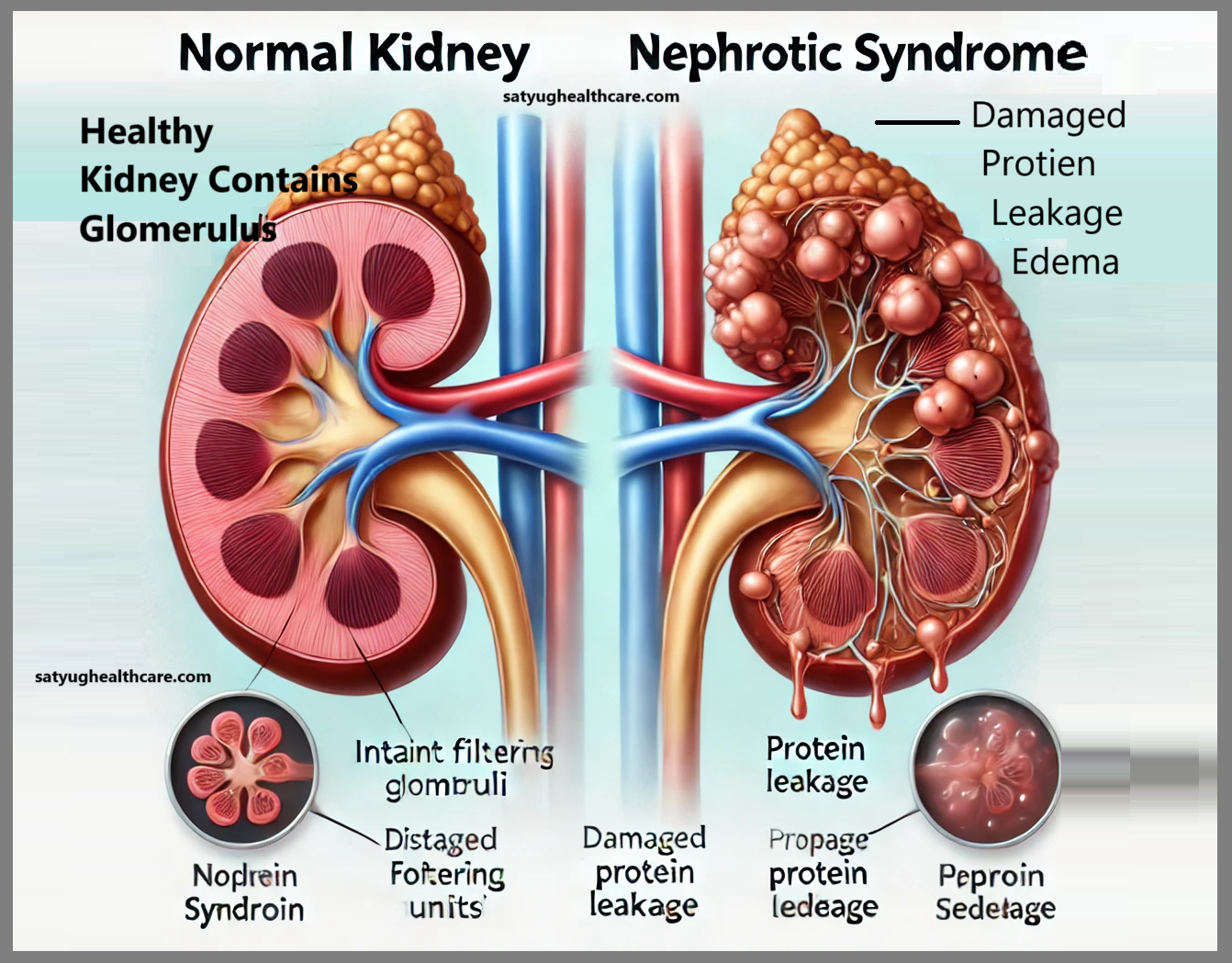
The dual usage of this term led to widespread confusion, prompting a consensus to define nephrotic syndrome exclusively in its second sense. It is now understood as the clinical condition marked by heavy proteinuria, hypoalbuminemia, and generalized edema. This definition implies that plasma albumin levels are reduced due to urinary albumin loss, and the resultant low plasma oncotic pressure alters Starling forces, leading to edema. These criteria are generally met when protein loss exceeds 5 grams daily and plasma albumin drops below 3 grams per 100 ml.
Importantly, the definition excludes features such as renal excretory failure, hypertension, and hypercholesterolemia. Attempts to include these elements have been abandoned in favor of a more streamlined definition. While hypercholesterolemia often accompanies nephrotic syndrome, its mechanism remains unclear, and its inclusion complicates the definition without providing diagnostic clarity.
Etiology of Nephrotic Syndrome
Nephrotic syndrome can be transient or persistent. Transient cases are usually of minor diagnostic and therapeutic concern, while persistent nephrotic syndrome presents significant challenges. In Europe and North America, approximately 75% of persistent cases are attributed to three idiopathic glomerular diseases:
1. Minimal Change Disease: The most common cause in children, accounting for one-fifth to one-third of adult cases.
2. Membranous Disease: Predominant in elderly men.
3. Chronic Proliferative Glomerulonephritis: Slightly more common than membranous disease.
The remaining 25% of cases result from secondary causes, such as:
• Diabetic glomerulosclerosis
• Amyloidosis
• Various forms of focal glomerulonephritis (e.g., lupus erythematosus, anaphylactoid purpura)
• Renal vein thrombosis
Clinical Manifestations
Edema is the hallmark of nephrotic syndrome. Generalized edema often extends to ascites and pleural effusions, driven by reduced plasma oncotic pressure due to hypoalbuminemia. Factors such as salt intake and mineralocorticoid activity also contribute. The severity of edema does not consistently correlate with plasma albumin levels.
In children, facial edema often appears early, whereas adults more commonly experience edema in the lower extremities. Severe cases can lead to a 50% increase in body weight due to fluid retention.
Hypertension is present in some patients, depending on the type of glomerular disease. Conversely, extremely low plasma volume caused by severe hypoalbuminemia can result in vascular collapse and hypotension. Protein malnutrition due to urinary protein losses may cause muscle wasting, often masked by generalized edema, or growth retardation in children. Additional signs include increased nail opacity (leukonychia), which can sometimes help estimate the duration of the condition.
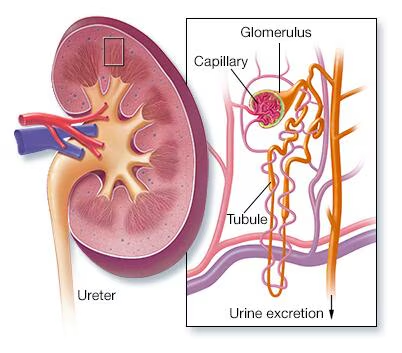
Urinary abnormalities include oliguria during edema accumulation and proteinuria exceeding 5 grams daily. The extent of renal impairment varies based on underlying pathology, and transient renal failure can occur due to hypovolemia or tubular damage, independent of destructive glomerular disease. In some pediatric cases, nephrotic syndrome manifests with renal glycosuria, aminoaciduria, and potassium loss due to tubular defects.
Biochemical Changes
Plasma albumin levels invariably drop below 3.0 grams per 100 ml, with levels as low as 0.5 grams per 100 ml in severe cases. Such extreme hypoalbuminemia often leads to hypovolemia and edema resistant to treatment. While other plasma proteins may remain normal, electrophoresis typically reveals decreased alpha and gamma globulins, increased alpha and beta globulins, and elevated fibrinogen levels.
Hyperlipidemia is another characteristic feature, involving all major plasma lipids, including cholesterol, triglycerides, and phospholipids. Plasma cholesterol levels can exceed 1500 mg per 100 ml, though these levels vary widely among patients. Hyperlipidemia’s mechanism remains unclear but is strongly associated with hypoalbuminemia. Nephrotic hyperlipidemia increases the risk of premature atherosclerosis.
Treatment Approaches
Management of Edema
Edema contributes significantly to morbidity and mortality, often leading to infections and complications from immobility. While low serum albumin is the primary cause of edema, there is no practical method to increase plasma albumin levels while urinary protein losses persist. High-protein diets, though sometimes marginally effective in raising albumin levels, often exacerbate proteinuria and are economically prohibitive for many patients.
Intravenous administration of salt-poor human albumin can be beneficial in hospital settings for patients with circulatory collapse due to hypovolemia or refractory edema, but its effects are transient and impractical for long-term management.
Diuretics are the cornerstone of edema treatment. Except in cases of severe hypoalbuminemia or renal failure, diuretics alone can typically control edema. Treatment usually begins with milder agents, such as thiazides, escalating to more potent drugs like furosemide or ethacrynic acid if needed. Potassium deficiency, a common side effect of diuretics, should be managed with potassium supplements or potassium-sparing diuretics like spironolactone or amiloride. In cases of advanced renal failure, potassium depletion is rare, and potassium-sparing agents should be avoided to prevent hyperkalemia.
Combining diuretics with a low-sodium diet (as low as 20 mEq daily) can expedite edema resolution but is generally unnecessary except in severe renal failure.
Addressing Hyperlipidemia
Although hyperlipidemia is a prominent feature, its management is secondary to treating the underlying glomerular disease. The relationship between lipid levels and hypoalbuminemia underscores the complexity of this condition, and further research is needed to clarify treatment strategies.
Specific Treatment of Glomerular Lesions
The treatment of underlying glomerular diseases causing nephrotic syndrome varies. While some conditions are refractory to treatment, exceptions exist and are addressed on a case-by-case basis. Comprehensive management requires addressing the primary glomerular pathology.
Traditional and Alternative Treatments
Ayurvedic medicine offers an alternative approach, emphasizing holistic healing through herbal remedies and techniques like pulse diagnosis. Proponents suggest that Ayurvedic treatments can effectively address nephrotic syndrome without invasive procedures, but further scientific validation is necessary to confirm these claims.
Nephrotic syndrome is a complex clinical condition requiring a nuanced approach to diagnosis and treatment. Understanding its underlying causes, clinical manifestations, and biochemical changes is essential for effective management. While conventional treatments focus on symptom control and addressing primary glomerular diseases, alternative therapies like Ayurveda may provide complementary options for patients seeking holistic care. Collaboration between medical disciplines could pave the way for improved outcomes in managing this challenging condition.
The views expressed in this article are solely those of the author and do not necessarily reflect the opinions or views of this Magazine. The author can be reached at 9650696341
Leave a Reply